11. Summer of Covid

June 13, 2020
It’s almost summer in Europe. COVID-19 seems to be a recent nightmare. Glad it’s over. But it isn’t, of course.
There are several ways in which it isn’t over:
- A second wave will probably hit Europe and the US in the autumn. It may be even much worse, given the pandemic of a century ago.
- Worldwide, the number of daily reported cases is still increasing week after week.
- COVID-19 is raging in other parts of the world. The disaster there may become much more prominent than in the more economically developed world.
- Other coronaviruses are probably finding their way to the same niche: stressful organisms, including us.
- We cannot exclude the possibility of a mutation of the virus that makes it more dangerous. See Spanish flu, 1918, death toll: 10-100 million.
- Part of the matter is the economic downfall: countries on the verge of collapse due to the first wave cannot take another blow. This may have huge secondary effects, such as populations getting on the move, especially with climate change as an accompanying disaster.
- An even more essential part of the matter is that this is about us, about the human being in general. Many illnesses are of the mind rather than exclusively the body. In COVID-19, the mind is being ignored in a truly insane way. That’s a pity. Seeing the mind in this issue may open eyes to its influence on many other matters, which are even more significant than COVID. Yes, I mean it when I write it.
The COVID-19 adventure may pass an entire planet without being taken as a wake-up call. At this moment, almost nowhere is the mind discussed as a potential element in the whirlpool. We now have a European summer as a resting point. That only lasts three months. Of course, other parts of the world don’t have this resting point, on the contrary! Let’s not wait.
Europe thinks it has been smart and (+/-) disciplined, so, virus (+/-) gone. A triumph of science? But the reality is very different from the show. We need science indeed, much more than we presently have. We need more rationality and, at the same time, more depth.
A coronavirus is different from an influenza-virus. But some common cold viruses are also of the corona type. We can look at the science about this. Interestingly, the influence of stress on common cold was investigated and proven already 30 years ago [Cohen et al., 1991]. This brings us eerily close to COVID-19.
Is the COVID-19 virus then no more dangerous than a regular flu virus? Hah, politically hazardous question. One can already hear knives being sharpened. Will he dare to write the unsayable? Well, no. COVID-19 is more dangerous than the flu. But if you could really take the whirlpool out of the picture, the difference might become substantially smaller. If, on top of this, one could use one’s mind in optimal ways, then I cannot confidently say that the difference would be significant. But since we are not there, the difference is clearly present. There is no denigration meant in this. It’s an admonition. What else can I say? Use your mind as cure. Combine it with every other means at your disposition.
Note that symptoms of common cold appear in autumn and winter. In May and during summertime, common colds are seldom. We see, accordingly, a diminishment of COVID-19 in ‘common cold countries.’ Probably, we have been lucky that the pandemic took off only in March/April, almost at the end of the influenza season. So, we may ask, have we indeed been lucky or is the COVID season constrained to the end-of-winter period? In the autumn, will the COVID-season show to be just displaced in time or is it more extensive than the influenza period? Will it show its full-blown presence from October till April? Will we have more deaths from corona than from influenza every year, even with vaccination? Those are some of the many things that we don’t know yet.
Do we win the ‘battle against influenza’ every year? No, the time of the year does it for us, until autumn strikes again. Experts are not unanimously convinced that this seasonality, as in the case of influenza, is mainly virus-related. Another hypothesis is that the observed seasonality of influenza is the result rather of a constant level of infection mediated differently by the host immune system over time. People may be susceptible to infection at different times of the year by pathogens which are present year-round. [Dowell SF., 2001] Complex networks of interactions among patients’ immune systems, society as a whole, weather conditions, and the continual adaptation of viral antigens to form new strains are probably responsible for seasonal flu infections. The elucidation of all this is by far not finished. A lot remains unexplained. Will the explanatory holes be filled rather by body or mind? Am I suggesting something inappropriate?
One thing is sure: the seasonal trend is very sharp. See this curve from https://www.cdc.gov/flu/about/season/flu-season.htm :

This is in the US, without influenza lockdown, nor social distancing and face masks. Note the disappearance in the summer and re-appearance in autumn-winter. Several other respiratory viruses also circulate during the flu season. Note that affective disorders can also be seasonal. [Kurlansik et al., 2012] Different parts of the world show different curves of viral infection. In some, there are no peaks but year-round activity.
Corona is different, but not that much. For instance, a recent study by the University of Michigan School of Public Health tracked a group of participants over 8 years, looking at the prevalence of the four most common human coronaviruses in the population. They concluded that coronaviruses are sharply seasonal, appearing to have similar transmission potential to influenza A in the same population. [Monto AS et al., 2020] The authors noted a peak aggregate month of all four coronaviruses between January and February. One of the four similar curves:
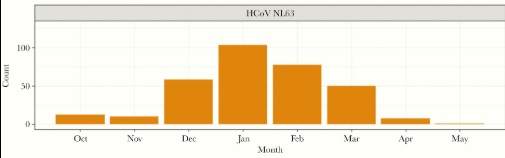
Other and prior studies have corroborated these results. [Killerby ME et al., 2018]
The point is that we did not win this battle, let alone the war, even though it may appear so at present, and we have been given this impression more or less. Virologists should not be chest-pounding (as many of them aren’t). To be honest, economic reasons also seem to play a significant role in how people in Europe are led to be confident that the worst is over. If so, then it would be very misguided and short-sighted. Especially the virologists can warn people much more openly for a second wave. It matters a big deal to know about this. In a few months from now till then, money can be spent differently, much more wisely, with this knowledge. But it is a politically tricky statement with a huge counterfactual risk involved. If speaking out helps, few people compare with the deadlier alternative. If part of the – even well-considered – gamble turns out badly, everybody indignantly knows. Here, true leadership is needed. This is what it’s for.
Brazil now has a coronavirus death toll of 42,720 fatalities, second only to the US. I take Brazil as an example of what happens in many other countries of Latin-America and more. We saw a Brazilian curve in a previous chapter. Let’s look at Egypt today as just another example (from https://www.worldometers.info/coronavirus):

So, in Brazil, with its hotter temperatures, it may be surprising that so many deaths are to be deployed, and given challenges of reporting, probably many more. Does that contradict seasonal influence and, thus, the idea of pending return in Europe + US in a few months?
Unfortunately not. As said, not only warmth is relevant in seasonality. A complex interplay of factors is responsible. In Brazil, we see an influenza season that peaks in June till August, plummeting in September. As said, corona is not influenza, but it’s not very much different in behavior (droplet-mode of infection). In this sense, it’s not surprising that it is surging now. The odds are that COVID-19 will be ravaging through the land till September. If it plummets then, we have another clear admonition to brace ourselves in Europe + the US, as the viral momentum will be regained in reverse to the South.
Has the first lockdown in many countries been for naught? Good question. I think the answer is ‘no.’ But lockdown comes at such a terrible price emotionally and economically – which is also health-related in several ways – that things may not be clear-cut. Responsible politicians have a difficult job of calibration. If they are truly responsible, we should be lenient to their mistakes. We should not ask for their omniscience, but only for their sincere commitment. The lockdown has not been for naught, but with more openness, it could have had a much better effect on people and businesses. I ask for a commitment to look into the matter from every possible angle.
My advice for the next period of possible lockdown is not to use panic as a means to make people cautious. Panic doesn’t last, and it creates whirlpool-energy. Don’t treat people like puppets on strings because that way, you make them into puppets on strings. They may resent afterward. Also, those who are by nature not prone to hanging on strings get a hard time being true to themselves. They may try to bring more common sense but – through the puppet-making – encounter much resistance. This way, decent voices get subdued and make way to populist messages. That’s not what anyone profoundly wants.
In case of a second wave, we have – hopefully – the incentive of social distancing, face masks, respirators in place, experience in ICU, and hopefully some effective medication. BUT nevertheless, if people get into a whirlpool of hysteria again, this may again necessitate a lockdown. There will again be many infections and deaths because probably again, the lockdown will come too late (in the West). There will again be a huge burden to healthcare workers. Will there again be white cloths of support hanging from windows? Super, but even better would be an avoidance of a considerable part of the disaster.
It is clear to me that, without proper subconceptual support, panic will strike again and with renewed vigor in Europe and the US after the summer. Having a clear idea about what has happened recently and may happen again rather soon (the whirlpool) can relieve the damage not with a factor 0.1, but, in my view, with a factor 10. That is said as quickly as anything. Clear insight is crucial.
Of equal importance is the way of communicating this. The recent past doesn’t make it easier. Lots of people have died with the primary cure being present – but not reachable – inside themselves. How sad can it be?
I can only say that I’ve tried – not well enough – to make it open, to ‘promote’ for instance my recently published book ‘Your Mind as Cure.’ This will haunt me for the rest of my life; thank you very much. I received a fair amount of backlash and negation.… In view of my credentials in several domains, I think I’m not less scientific than any of my medical colleagues. Many prefer zero-tolerance in personal risk. It is, of course, never too late for this.
So, how to communicate this in a world that is caught in a basic cognitive illusion of not-seeing one’s depth and its influence on many things? The difficulty lies in how to combine an admonition to not get panicky with avoiding additional negative emotions of resentment and guilt. Public communicators might take additional coaching-lessons in this.
This does not mean that the conceptual defense (everything that is now regarded as to be done against the virus) should be abolished or even diminished. On the contrary, if COVID-19 comes haunting us again, we need to go for the full Monty, and well soon enough. That lesson has been learned once.
It’s even more important since a second wave will come with crowds being less motivated to be locked down. The first time, the puppets accepted the strings, having +/- total confidence in experts. The second time, patience may run dry. Expert-distrust may surge. The puppets may cut themselves loose and get into even more whirlpoolian trouble. Then what? I do expect that IF social trust in being able to win ‘the battle against COVID’ reaches some low point, the whirlpool will become re-enacted. Once it does so, we are in for a complete cycle: draconian measures to rebuild trust. That will – in the if situation – surely happen again, but will trust be restored before May 2021? In non-European/US countries too, the same phenomenon seems to play a substantial role. It may be less, or with a time-lag, but horrible stories reach smartphones everywhere.
About vaccination: Seven billion takes some time. So, who will get it first? The lack of vaccination in poor regions may enhance distrust and become fuel in the whirlpool. Resulting tensions will be felt at all sides. Moreover, people who take influenza vaccine shots at present notice that each year, they need another shot. That’s because the flu virus continuously mutates. This coronavirus also mutates continually, hopefully not as quickly. If it doesn’t diminish in virulence and fatality rate, then we’re in for a very long time.
The general communication about ‘final exit’ is that this will happen in the way of developing the vaccine, and that’s it. Of course, it needs to be made in huge quantities (billions?). We could live with that. But It’s not the end of the story. A vaccination against COVID-19 will most probably not be like the one against polio, but more like the one against influenza. We will need (expensive) vaccinations again and again.
More troubling, vaccination will not provide total immunity. The general communication appears to be: Being vaccinated makes one safe. It doesn’t work that way with every virus and probably also not with this one. It doesn’t make you safe, only safer. We may compare with influenza. Note that despite an existing (ongoing) vaccination, every year still sees 100.000s of fatalities. Quoting from the Centers for Disease Control and Prevention (https://www.cdc.gov/flu/vaccines-work/vaccineeffect.htm): “While vaccine effectiveness (VE) can vary, recent studies show that flu vaccination reduces the risk of flu illness by between 40% and 60% among the overall population during seasons when most circulating flu viruses are well-matched to the flu vaccine.” From another report (https://www.cdc.gov/mmwr/volumes/69/wr/mm6907a1.htm): “According to data from the U.S. Influenza Vaccine Effectiveness Network on 4,112 children and adults with acute respiratory illness during October 23, 2019–January 25, 2020, the overall estimated effectiveness of seasonal influenza vaccine for preventing medically attended, laboratory-confirmed influenza virus infection was 45%.” So, not 100% but around half of that. This makes a huge difference: many deaths, continuous anxiety, and an ever returning discussion about whether or not to go into lockdown (soon enough). On top of that, every mass vaccination leads to side effect, including some mortality through the vaccination itself. So, to what extent are we going to take this risk by giving it to younger people in order to disproportionately protect the older?
Interestingly with respect to vaccination is also the research about how the mind may affect the efficacy of vaccination against several viruses. [Yang et al., 2002], [Zimmermann et al., 2019], [Godbout et al., 2006] In general, acute stress heightens the response, chronic stress lowers it. What about acute upon chronic stress? Acute vs. chronic is a crude distinction. The more relevant distinctions we make, the more the phenomenon of ‘stress’ appears to be connected. My conclusion is that mind and vaccination are not two separate worlds. Moreover, having the one in place does not make the other unnecessary. We definitely need both.
Lately, Iran shows that a second wave is possible, probably not as only the result of better testing, but rather of easing the lockdown. The curve of daily cases at 16th of June (from https://www.worldometers.info/coronavirus), with deaths also rising as expected in the last few days:

How likely is a huge second wave in Europe and the US in case no wonder drug or procedure would come along? ‘Huge’ may be defined as: provoking at least as many deaths as until now, despite renewed lockdown and other conceptual measures. That is, with realistic counting, at least a million deaths worldwide, of which 320.000 in Europe+US. Nobody knows, so what are arguments for and against? Listing some:
- Things can quickly drastically change, as seems to have been partly forgotten at present. We just collectively experienced an example that we didn’t imagine possible five months ago. The fact that it has happened points to the probability of happening again.
- Other coronaviruses are among the common cold viruses. These show a clear seasonality: little to no presence in the summer, very much in wintertime. Top months are January – February. We have been lucky in 2020 that infections started going at full force only in March – April. Typically, the corona presence is already sharply declining by then.
- Until now, seasonality in other parts of the world is compatible with the prior point.
- Natural herd immunity is still very low at +/- 6%. This is: Almost everyone can still become infected and ill.
- Each year, the common colds reappear with somewhat changed, mutated viruses. A one-time immunity is not enough. The present coronavirus is likely to act like other coronaviruses and influenza.
- Immunity to other coronaviruses mostly lasts 6-12 months post-infection. Thus, people who got COVID-19 in the spring might get it again in the autumn or winter.
- Autumn and winter will come with the usual influenza epidemic. COVID will come on top of this with many people weakened by flu.
- More people will start thinking this is with us forever. Many will become depressed and may just ‘give up.’ Also, they may become less cautious for themselves and others before getting clinically depressed.
- The trust in experts may be much lower next time, making it harder to impose a new lockdown (soon enough). Economic arguments will also be much harsher.
- Vaccination, if and when attained, will probably work at +/- 50% efficacy.
- As to antiviral medication: Hopes are high; realizations poor until now. There may be a breakthrough.
- There will be no shortage of facemasks, hopefully.
- In-hospital mortality has declined over the months for patients with the same symptomatology, due to gathered medical experience.
- China contained the virus through draconian measures that are not possible in the West. Also, a small upsurge in China meets quick and decisive action through local lockdowns. Most probably, Western countries will be too slow.
- The Spanish flu of 1918 showed quite a hefty influenza epidemic in spring. The second wave came in autumn with much more force and mortality than caused by four years of WWI.
- Arguably, the stress levels of many people worldwide will be higher than ever due to social and economic evolutions. Adding to the whirlpool will be (social) media sowing panic about the second wave. Moreover, many people will still suffer from post-traumatic stress from the first wave experiences.
- There’s an increasing risk of another coronavirus. There have been three new ones in the last two decades. Before that, there may have been only a few more in two millennia.
Wonder drugs may come along. Hopefully, they do. Just now, dexamethasone is in the news, although not yet in scientific publications, nor have data sets been made available for other researchers to scrutinize. But it seems wonderfully good news indeed. This will probably become part of standard COVID therapy. Worrying may be a side effect of dexamethasone: it heightens psychotic delirium. As it happens, patients with severe COVID – when dexamethasone may become most indicated – frequently suffer from altered mental states or delirium, with rates of up to 70% in cases of severe illness. [O’Hanlon et al., 2020] Occasional descriptions are of a kind of prolonged bad trip through taking drugs. Some patients talk of preferring to die. Some need to be restrained. Antipsychotic treatment for hospital delirium shows a lack of efficacy and potential for adverse outcomes. [Nikooie et al., 2019] Non-pharmacological approaches (reorienting communication, early mobilization, therapeutic activities) are difficult to administer in the elderly [Hshieh et al., 2018] and, as a matter of fact, especially in cases of COVID. Also, this doesn’t end with getting better bodily. In some (many?) cases, it even gets worse when the patient is dismissed from the hospital. Little attention goes to this, but it may be a big problem. One should not only look at the deceased but also at the survivors.
Of course, this or any other wonder drug should not diminish the attention for the mind. In this case, as dexamethasone works through its influence on the immune system, it should even heighten such attention. The whole domain of psychoneuroimmunology shows that the mind and the immune system are very much intertwined. In future proper management of COVID – as in all of medicine – the mind and the body should be seen as the unity they are. One should say: the unity that it is. Looking at the human being as one unity of body and mind brings a much more positive story. For instance, referring to the app that you encounter at the beginning and the end of this book, I see a combination with dexamethasone as more than just a summation of both. On the one hand, within their mental exercises, users can integrate any idea of possible support and use it positively. On the other hand, having used the app and (still?) needing dexamethasone, they may be stronger to deal with a mental whirlpool that could otherwise push them into psychotic delirium.
Meanwhile, new studies are appearing that show the importance of the mind in relation to COVID. One excellent study showed the influence of COVID-related anxiety upon psychosomatic symptoms and disease. This is no surprise. The same influence acts upon the immune system in general, thus also on COVID-progression, closing this cycle in the whirlpool. [Shevlin et al., 2020 ]
Fortunately, taking mind seriously, a lot can be done. But it may take either sufficient investment in software or many human resources. The Aurelis-app ‘Acute stress’ is one element.
Human depth doesn’t cost anything by itself. That’s because it is not valued and doesn’t neatly come in packages. This summer and afterward, it may have the most significant Return On Investment of any time, in human health, lives and the economy, if we take action in due time.
Which is, of course, as soon as possible.
References
[Cohen et al., 1991] Cohen, S., G.M. Williamson, ‘Stress and infectious disease in humans,’ in: Psychol. Bull., 1991 (109), p. 5-24.
[Dowell SF., 2001] Dowell SF. Seasonal variation in host susceptibility and cycles of certain infectious diseases. Emerg Infect Dis. 2001;7(3):369‐374. doi:10.3201/eid0703.010301
[Godbout et al., 2006] Godbout JP, Glaser R. Stress-induced immune dysregulation: implications for wound healing, infectious disease and cancer. J Neuroimmune Pharmacol. 2006;1(4):421–427.
[Hshieh et al., 2018] Hshieh TT, Inouye SK, Oh ES. Delirium in the Elderly. Psychiatr Clin North Am. 2018;41(1):1-17. doi:10.1016/j.psc.2017.10.001
[Killerby ME et al., 2018] Killerby ME, Biggs HM, Haynes A, et al. Human coronavirus circulation in the United States 2014-2017. J Clin Virol. 2018;101:52-56. doi:10.1016/j.jcv.2018.01.019
[Kurlansik et al., 2012] Kurlansik SL, Ibay AD. Seasonal affective disorder. Am Fam Physician. 2012;86(11):1037‐1041.
[Monto AS et al., 2020] Monto AS, DeJonge P, Callear AP, et al. Coronavirus occurrence and transmission over 8 years in the HIVE cohort of households in Michigan. J Infect Dis. 2020;jiaa161. doi:10.1093/infdis/jiaa161
[Nikooie et al., 2019] Nikooie R, Neufeld KJ, Oh ES, et al. Antipsychotics for Treating Delirium in Hospitalized Adults: A Systematic Review. Ann Intern Med. 2019;171(7):485-495. doi:10.7326/M19-1860
[O’Hanlon S et al., 2020] O’Hanlon S, Inouye SK. Delirium: a missing piece in the COVID-19 pandemic puzzle [published online ahead of print, 2020 May 6]. Age Ageing. 2020;afaa094. doi:10.1093/ageing/afaa094
[Shevlin et al., 2020 ] Shevlin M, Nolan E, Owczarek M, et al. COVID-19-related anxiety predicts somatic symptoms in the UK population [published online ahead of print, 2020 May 27]. Br J Health Psychol. 2020;10.1111/bjhp.12430. doi:10.1111/bjhp.12430
[Yang et al., 2002] Yang EV, Glaser R. Stress-associated immunomodulation and its implications for responses to vaccination. Expert Rev Vaccines. 2002;1(4):453‐459. doi:10.1586/14760584.1.4.453
[Zimmermann et al., 2019] Zimmermann P, Curtis N. Factors That Influence the Immune Response to Vaccination. Clin Microbiol Rev. 2019;32(2):e00084-18. Published 2019 Mar 13. doi:10.1128/CMR.00084-18
Related Posts

Where is/was the Mind in COVID-19 Causality?
This is the title of an article – by me – in the high-level medical journal ‘Brain, Behavior, & Immunity – Health,’ edition May 2022. With pain and all due respect, I dedicate it to the 18 million COVID mortality worldwide ― according to this recent publication in Nature magazine. Because of more naturalistic measurements, Read the full article…
5. What To Do in Times of Covid
Nothing worse than a false sense of security. Please, take every measure of precaution. Then, read on. March 30, 2020 This article can be read on its own. For more background, kindly follow this trail: Covid-19: Pandemia or Global Hysteria? Mind and Corona The Message in the Virus Covid and Attention [Recommendation: if Read the full article…
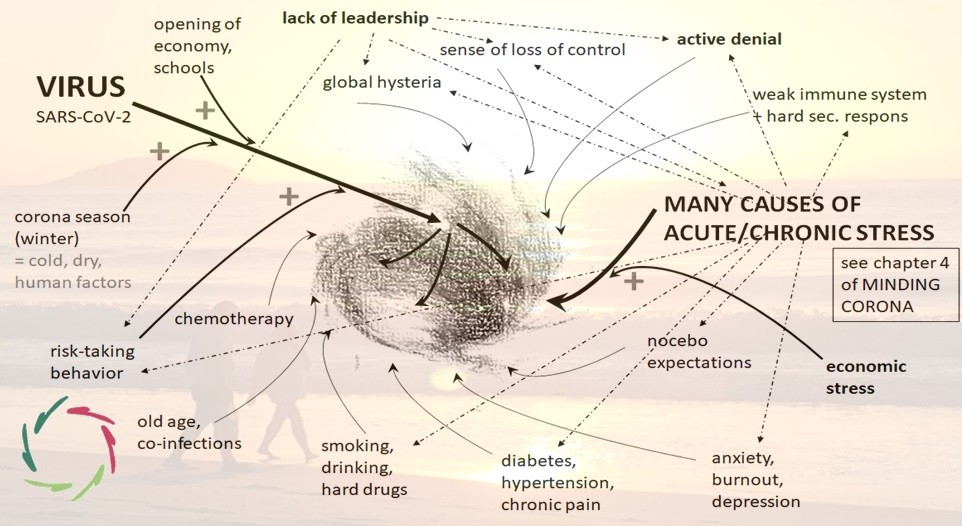
8 COVID-Whirlpool – In Which Virus AND Mind Play Substantial Roles
April 27, 2020 I expand upon an idea about what happens to a person getting more and more COVID symptoms towards a whirlpool that may become fatal. A whirlpool scenario probably happens in many cases of illness. It corresponds with complexity and multi-causal thinking. In crash-course: put many elements together, add more and more Read the full article…